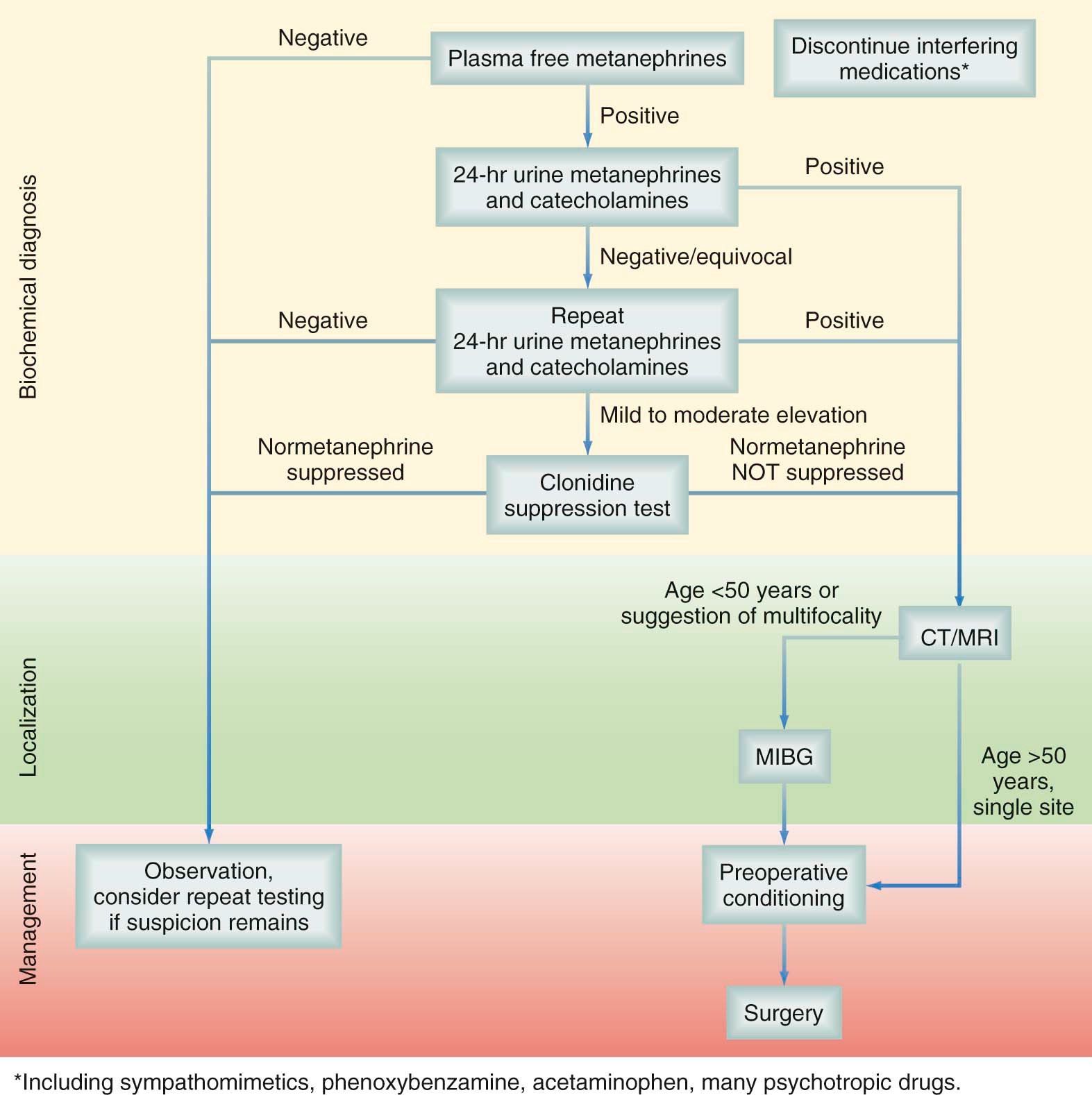
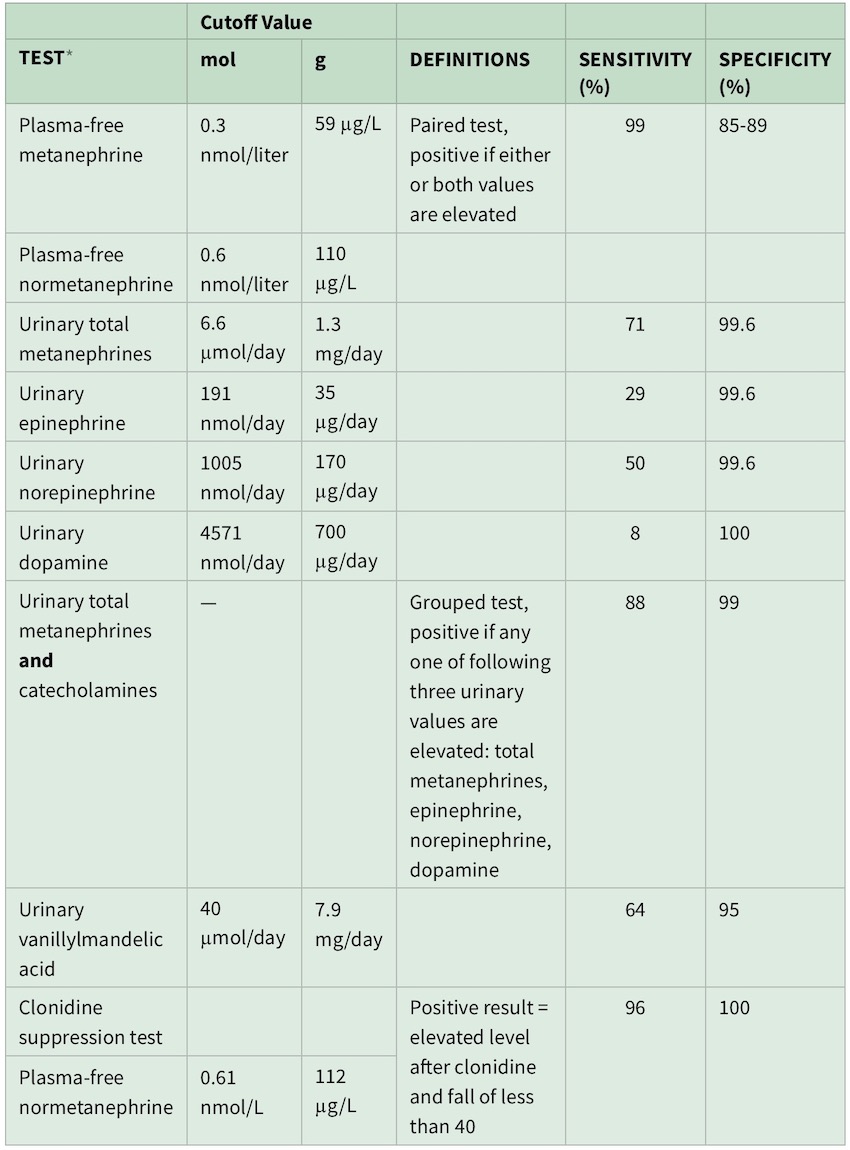
Sensitivities and specificities of these biochemical tests are dependent on the cutoff value used (greater than twofold to fourfold of the upper limit of normal) and whether the patient has a hereditary predisposition for pheochromocytoma. Plasma metanephrine should be drawn in a supine position and after an overnight fast to reduce the likelihood of false-positive results from increased levels resulting from upright posture or caffeine and nicotine use Acetaminophen, labetalol, sotalol, alpha-methyldopa, tricyclic antidepressants, buspirone, phenoxybenzamine, monoamine oxidase (MAO) inhibitors, sympathomimetics, cocaine, sulfasalazine, and levodopa, that can cause falsely elevated levels of plasma and urinary metanephrine and normetanephrine. Tests performed during episodes of acute pain, critical illness, or urgent hospitalization may be misleading Plasma-free metanephrine testing carries an extremely high sensitivity, approaching 99%, and, being a one-time blood test, is more convenient than 24-hour urine testing. Specificity however is only 89% at best. The primary usefulness of plasma-free metanephrine testing is to exclude pheochromocytoma when the test is negative When serum metanephrines are positive, confirmatory testing with 24-hour urine levels of catecholamines and their metabolites is required A urine collection may be considered positive if total metanephrines or any single catecholamine fraction (e.g., epinephrine, norepinephrine, dopamine) is elevated above its cutoff value | 











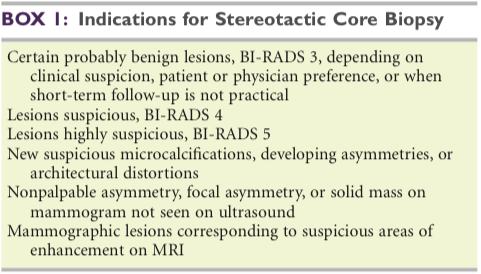
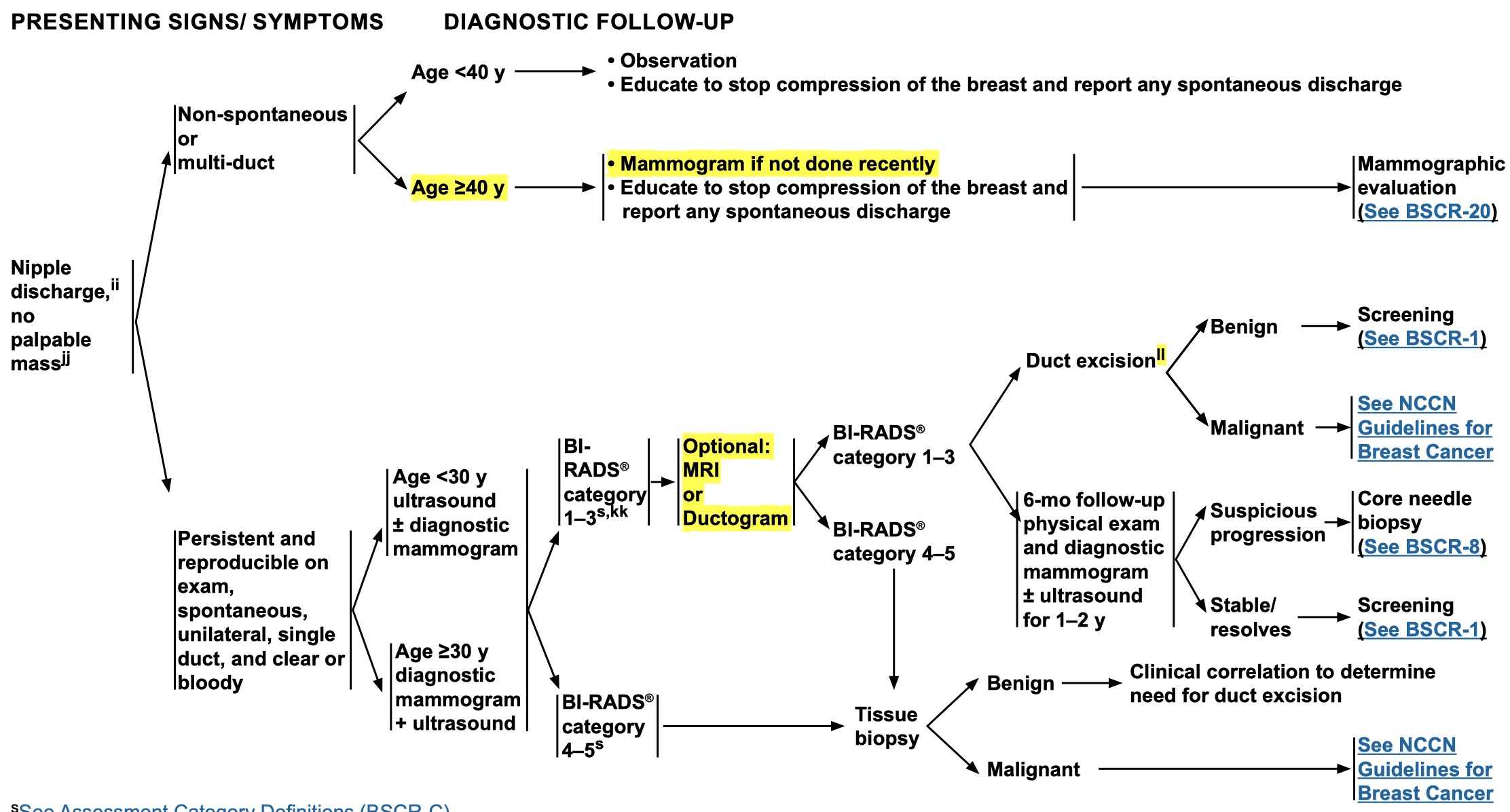 ll: Based on clinical suspicion and patient preference.
ll: Based on clinical suspicion and patient preference.